Nephrotic syndrome secondary to focal segmental glomerulosclerosis in a patient with controlled HIV
A case report.
DOI:
https://doi.org/10.56867/172Keywords:
Síndrome nefrótico secundario, Glomeruloesclerosis focal y segmentaria, VIH, Reporte de casoAbstract
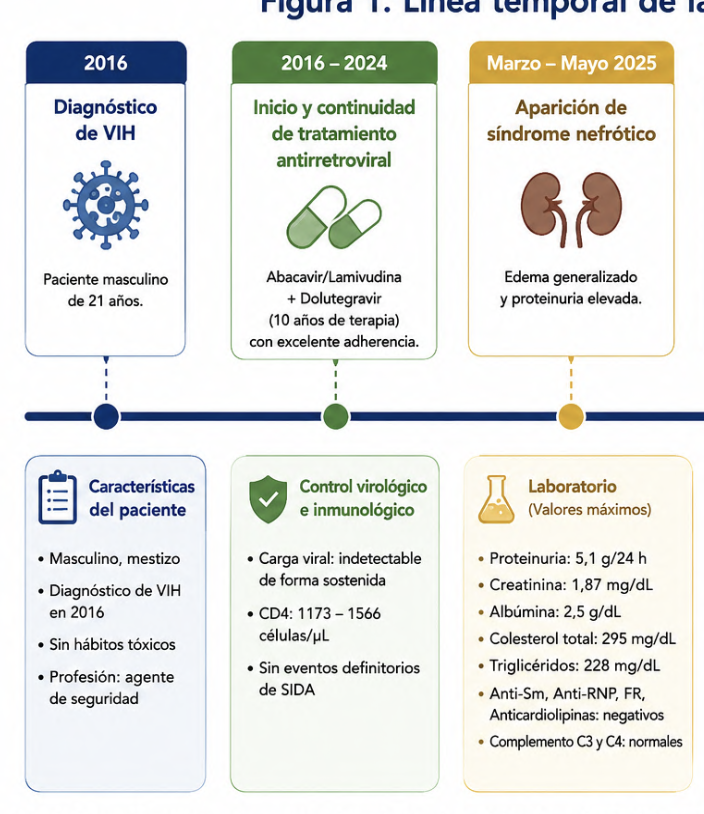
Introduction: Focal segmental glomerulosclerosis (FSGS) is a leading cause of nephrotic syndrome in adults and contributes significantly to the progression of chronic kidney disease. In patients with HIV infection, glomerulopathies are typically associated with active viral replication and immune deterioration; however, their occurrence in individuals with sustained virologic suppression poses a diagnostic and therapeutic challenge. We present the case of a young patient with controlled HIV who developed nephrotic syndrome secondary to biopsy-confirmed FSGS.
Case report: We report the case of a 31-year-old mixed-race man with a history of HIV infection since 2016, on continuous treatment with abacavir/lamivudine and dolutegravir, with a persistently undetectable viral load and adequate immune reconstitution. Medical history, laboratory tests, renal ultrasound, and renal biopsy findings were reviewed to establish the diagnosis and initiate treatment.
Results: The patient presented with nephrotic-range proteinuria (5.1 g/24 h), creatinine levels between 1.46 and 1.87 mg/dL, and an immunological profile negative for autoimmune diseases. Ultrasound showed kidneys of preserved size with altered corticomedullary echogenicity and bilateral non-obstructive lithiasis. Renal biopsy confirmed FSGS with interstitial fibrosis and mild tubular atrophy (20%). Treatment with losartan, spironolactone, empagliflozin, prednisone, and tacrolimus was initiated while maintaining antiretroviral therapy; the patient maintained an undetectable viral load and immunological stability.
Conclusions: FSGS can occur in patients with adequately controlled HIV infection, even in the absence of viral replication and with high CD4 lymphocyte counts, although this presentation is less common than classic HIV-associated nephropathy (2–4). The renal biopsy was crucial for establishing the diagnosis and guiding immunosuppressive treatment, highlighting the importance of considering other etiologies of nephrotic syndrome in people with HIV and conducting a comprehensive nephrological evaluation to optimize management and preserve renal function (1,4).
Published
Issue
Section
License
Copyright (c) 2026 Karla Amanda Manzano Bayas, Karla Gabriela Ramos Burgos, Nieve Karina Peña Ponce (Author)

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
